What is Deep Brain Stimulation?
NuRaX is a leader in the treatment of movement disorders, which include Parkinson's disease, Essential tremor, Dystonia, Huntington Chorea, Epilepsy, Obsessive Compulsive disorders and Treatment Resistant Depression. In collaboration with premier hospitals, we perform maximum numbers of Deep Brain Stimulation (DBS) surgeries a year, with capabilities to perform DBS surgery while patients are asleep or awake.
Deep Brain Stimulation (DBS) is a pain-free surgical procedure to implant a device that sends electrical signals to brain areas responsible for body movement. Electrodes are placed deep in the brain and are connected to a stimulator device. Similar to a heart pacemaker, a neurostimulator uses electric pulses to regulate brain activity. DBS can help reduce the symptoms of tremor, slowness, stiffness, and walking problems caused by Parkinson's disease, dystonia, or essential tremor.
.jpg)
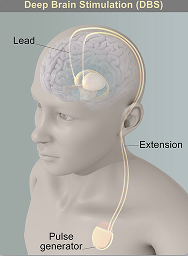
A DBS system has three parts implanted inside the body:
Neurostimulator — a programmable battery-powered pacemaker device that creates electric pulses. It is placed under the skin of the chest below the collarbone or in the abdomen.
Lead — a coated wire with a number of electrodes at the tip that deliver electric pulses to the brain tissue. It is placed inside the brain and connects to an extension wire through a small hole in the skull.
Extension — an insulated wire that connects the lead to the neurostimulator. It is placed under the skin and runs from the scalp, behind the ear, down the neck, and to the chest.
The patient uses a handheld controller to turn the DBS system on and off. The doctor programs the stimulator settings with a wireless device. Unlike other surgeries such as pallidotomy or thalamotomy, DBS does not damage the brain tissue. Thus, if better treatments develop in the future, the DBS procedure can be reversed.
Electrode Placement Sites
Normal muscle tone, movement, timing, and coordination depend on complex electrical circuits or feedback loops in the brain. The basal ganglia are responsible for activating and inhibiting these feedback loops. In Parkinson's, parts of the basal ganglia are either under- or over-stimulated. DBS of specific ganglia alters the abnormal electrical circuits and helps stabilize the feedback loops, thus reducing symptoms.
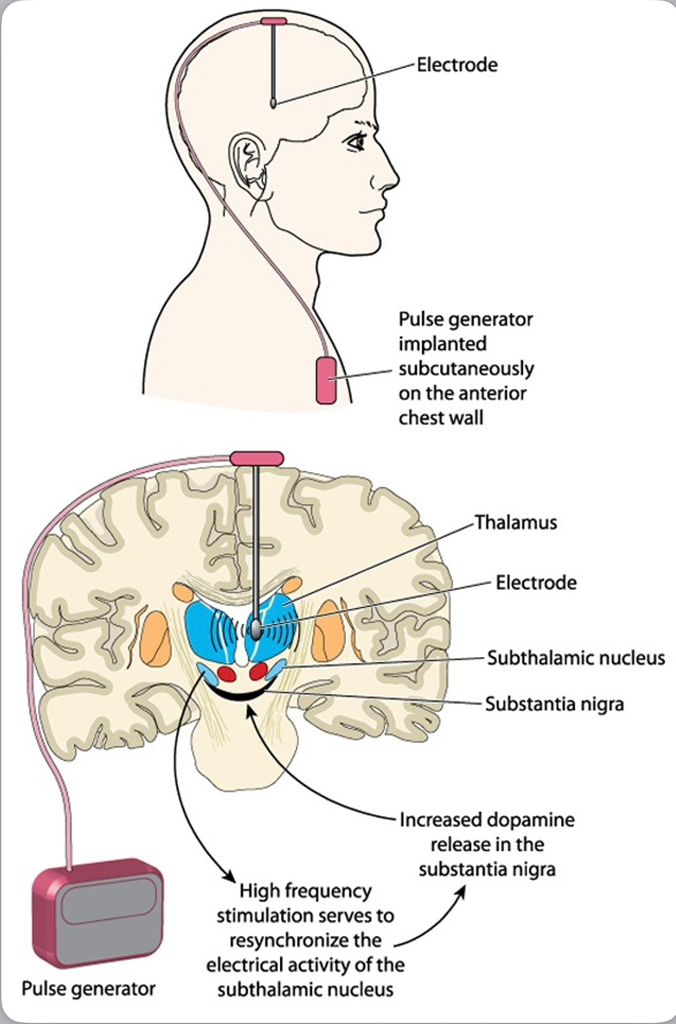
Electrodes can be placed in the following brain areas:
- Subthalamic nucleus (STN) — effective for tremor, slowness, rigidity, dystonia and dyskinesia. Most commonly used to treat Parkinson's disease.
- Thalamus (VIM) — effective for tremor. It is often used to treat essential tremor.
- Globus pallidus (GPi) — effective for tremor, slowness, rigidity, dystonia and dyskinesia. It is used to treat dystonia and Parkinson's disease.
Who is a Candidate?
You may be a candidate for DBS if you have:
- A movement disorder with worsening symptoms (tremor, stiffness) and your medications have begun to lose effectiveness.
- Troubling "off" periods when your medication wears off before the next dose can be taken.
- Troubling "on" periods when you develop medication-induced dyskinesias (excessive wiggling of the torso, head, and/or limbs).
DBS can help treat many of the symptoms caused by the following conditions:
- Parkinson's disease: tremor, rigidity, and slowness of movement caused by the death of dopamine-producing nerve cells.
- Essential tremor: involuntary rhythmic tremors of the hands and arms, occurring both at rest and during purposeful movement.
- Dystonia: involuntary movements and prolonged muscle contraction, resulting in twisting body motions, tremor, and abnormal posture.
- Obsessive-Compulsive Disorder (OCD)
- Drug-Resistant Epilepsy
- Chronic Pain Syndromes
The Surgical Process
DBS surgery is performed by a Neurosurgeon who has specialized training in Functional Neurosurgery. The surgical team also includes a Neurologist and Neuromodulation Specialist. The procedure follows a carefully planned, multi-step process:
Attach Stereotactic Frame
The frame is temporarily positioned on your head with Velcro straps. The four pin sites are injected with local anaesthesia to minimize discomfort. You will feel some pressure as the pins are tightened.
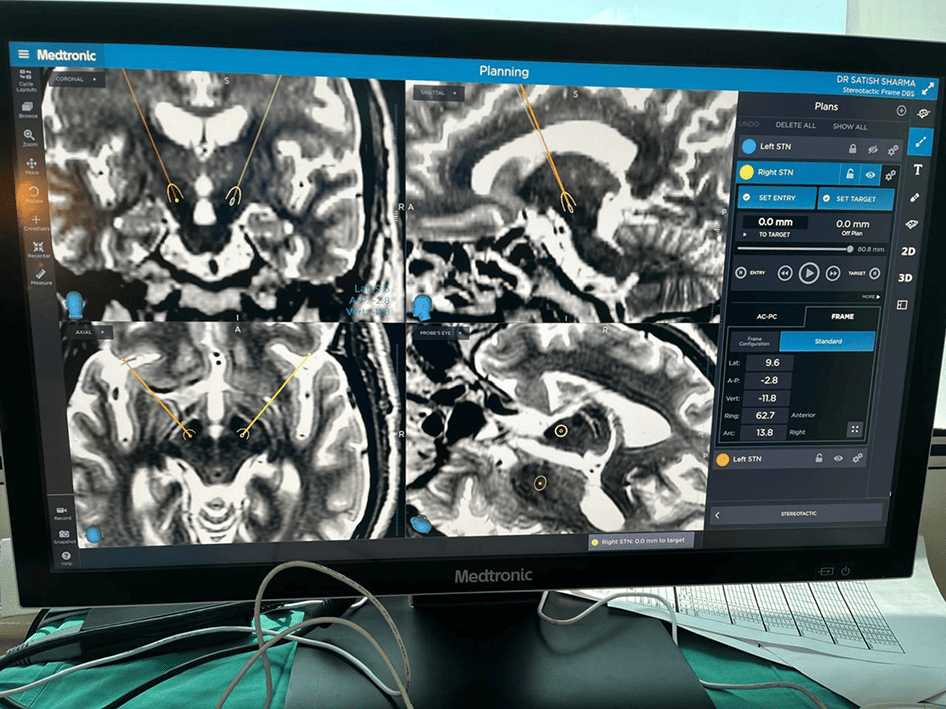
MRI or CT Scan
A box-shaped localizing device is placed over the frame. Markers help pinpoint the exact three-dimensional coordinates of the target area within the brain. The surgeon uses the MRI/CT scans and special computer software to plan the trajectory of the electrode.
Skin and Skull Incision
You will remain awake during surgery. Light sedation is given for the initial incision, then stopped so you can talk to doctors and perform tasks. A skin incision is made across the top of the head to expose the skull, and two quarter-sized burr holes are drilled.
Insert Electrode in the Brain
A recording electrode is inserted to a precise depth and angle. The brain itself does not feel pain. Accuracy is confirmed by asking you to lift your arms, legs, or count numbers. The team also listens for correct nerve cells using computer waveforms. This must be repeated for both sides of the brain.
Test Stimulation
Once the exact nerve cells are located, the surgeon replaces the recording electrode with a permanent DBS electrode/lead. Test stimulation is performed and you will be asked if you feel any of your symptoms lessen or completely go away.
Closure
A plastic cap is placed over the burr hole to hold the lead in place. A coil of wire is left under the scalp for later attachment to the extension wire and stimulator. The scalp incision is closed with sutures or staples.
Implant the Stimulator
In a separate procedure under general anaesthesia, a small incision is made near the collarbone and the neurostimulator is implanted under the skin. The lead is attached to an extension wire that is passed under the skin of the scalp, down the neck, to the stimulator in the chest or abdomen.
Program the Stimulator
About 10 days after surgery, the stimulator is programmed and medication dosage adjusted. You may be asked to stop medications for up to 12 hours before programming. Returns every 3 weeks; typically 3-4 sessions are needed for maximum symptom control while minimizing side effects.
Awake vs. Asleep DBS Surgery
Standard DBS surgery is performed while you are awake and requires stopping the medicines that control your Parkinson's symptoms. During surgery, you are asked to perform tasks to help guide the electrode to the precise location in the brain. Being awake during brain surgery, or being off medicine, is unsettling for some people.
Asleep DBS is an alternative option at some centres. The surgery is performed while you are unconscious and under anaesthesia, taking place in an MRI or CT scanner to target and verify accurate placement of your DBS electrodes.
Results and Outcomes
For Parkinson's disease, DBS of the subthalamic nucleus improves the symptoms of slowness, tremor, and rigidity in about 90% of patients. Most people are able to reduce their medications and lessen side effects, including dyskinesias. It has also been shown to be superior in long-term management of symptoms than medications alone.
For essential tremor, DBS of the thalamus as well as the Subthalamic Nucleus may significantly reduce hand tremor in 80 to 90% of patients and may improve head and voice tremor.
DBS of the globus pallidus (GPi) is most useful in treatment of dyskinesias (involuntary wiggly movements), dystonias, as well as other tremors. Patients also report additional benefits such as better sleep, more involvement in physical activity, and improved quality of life.
Risks and Considerations
No surgery is without risks. General complications of any surgery include bleeding, infection, blood clots, and reactions to anaesthesia. Complications related to placement of the DBS lead include seizures, infection, and a 1% chance of bleeding in the brain.
Reasons for additional surgery may include breakage of the extension wire in the neck, parts wearing through the skin, or removal due to infection or mechanical failure. The battery will need to be replaced every 4 to 5 years. Some DBS systems have a rechargeable battery that may last up to 15 to 25 years.
DBS may also cause worsening of some symptoms such as speech and balance impairments. In some patients with Parkinson's, DBS may cause or worsen depression. If you develop any side effects from a stimulation adjustment, you need to return to the office for further programming.
Living with a Stimulator
Once the DBS has been programmed, you are sent home with instructions for adjusting your own stimulation. The handheld controller allows you to turn the stimulator on and off, select programs, and adjust the strength of the stimulation. Most patients keep their DBS system turned on 24 hours day and night. Some patients with essential tremor can use it during the day and turn off the system before bedtime.
If your DBS has a rechargeable battery, you will need to use a charging unit. On average, charging time is 1 to 2 hours per week. Just like a cardiac pacemaker, other devices such as cellular phones, pagers, microwaves, security doors, and anti-theft sensors will not affect your stimulator. Be sure to carry your Implanted Device Identification card when flying, since the device is detected at airport security gates.
Latest Case Studies





Why Choose NuRaX for DBS
NuRaX offers one of the most experienced DBS programs in the world, bringing together unparalleled expertise and comprehensive patient care:
- Over 600 DBS procedures performed by Dr. Albert J. Fenoy, one of the most experienced DBS neurosurgeons globally.
- Advanced neuroimaging guidance using state-of-the-art MRI, CT, and intraoperative neurophysiology for precise electrode placement.
- Multidisciplinary team approach with neurologists, neurosurgeons, neuropsychologists, and rehabilitation specialists collaborating on every case.
- Awake and Asleep DBS options available to suit patient needs and comfort levels.
- International patient coordination with experience treating patients from over 10 countries, providing comprehensive travel and care logistics support.
Glossary
- Basal Ganglia
- Mass of nerve cell bodies located deep within the white matter of the cerebrum; controls movement subconsciously.
- Bradykinesia
- Slowness of movement, impaired dexterity, decreased blinking, drooling, expressionless face.
- Dopamine
- A neurotransmitter that passes messages between neurons across a synapse; essential for movement regulation.
- Dyskinesia
- Abnormal involuntary movements that can be caused by high or low levels of anti-Parkinson medication.
- Globus Pallidus Interna (GPi)
- Nuclei that regulate muscle tone; part of the basal ganglia. A DBS target for dystonia and Parkinson's.
- Stereotactic
- A precise method for locating deep brain structures using 3D coordinates derived from MRI or CT imaging.
- Subthalamic Nucleus (STN)
- The most common DBS target for Parkinson's disease; regulates movement-related signals.
- Substantia Nigra
- Brain area where dopamine is produced; degeneration of this region causes Parkinson's disease.
- Thalamus
- Relay station for sensory messages entering the brain; the VIM nucleus is a DBS target for essential tremor.
References
- Deep-Brain Stimulation for Parkinson's Disease Study Group. N Engl J Med 345:956-63, 2001.
- Weaver FM, Follett K, et al. Bilateral Deep Brain Stimulation vs Best Medical Therapy for Patients With Advanced Parkinson Disease. JAMA 301:63-73, 2009.
- Deuschl G, Schade-Brittinger C, et al. A Randomized Trial of Deep-Brain Stimulation for Parkinson's Disease. N Engl J Med 355:896-908, 2006.
- Spieles-Engemann AL, et al. Stimulation of the rat subthalamic nucleus is neuroprotective following significant nigral dopamine neuron loss. Neurobiol Dis 39(1):105-15, 2010.